

Current Understanding of the Potential Mechanism of Action of the Investigational Therapy Multikine® (Leukocyte Interleukin, Injection)
Multikine (Leukocyte Interleukin, Injection) is the full name of this investigational therapy, which, for simplicity, is referred to in the remainder of this page as Multikine*. Multikine has not been licensed or approved for sale, barter or exchange by the FDA or by any other regulatory agency.
Data from the Phase III study in support of the understanding of the mechanism of action (MOA) of Multikine will be published in peer-reviewed journals. Phase II data leading to our understanding of the mechanism of action (MOA) of Multikine was published in peer reviewed journals (Timar et all Laryngoscope 2003 and JCO 2005). Clinical and pathology data from Phase 1 and Phase 2 clinical trials with the Multikine investigational immunotherapy was published in peer-reviewed scientific journals (Feinmesser et al Arch Otolaryngol. Surg. 2003; Timar et al 2003 and 2005) suggest that Multikine has the potential to produce an anti-tumor response, as the reported data from these early-stage studies suggests:
- Multikine potentially may recognize and/or bind to multiple (different) antigens (or receptors) on the cancer cells.
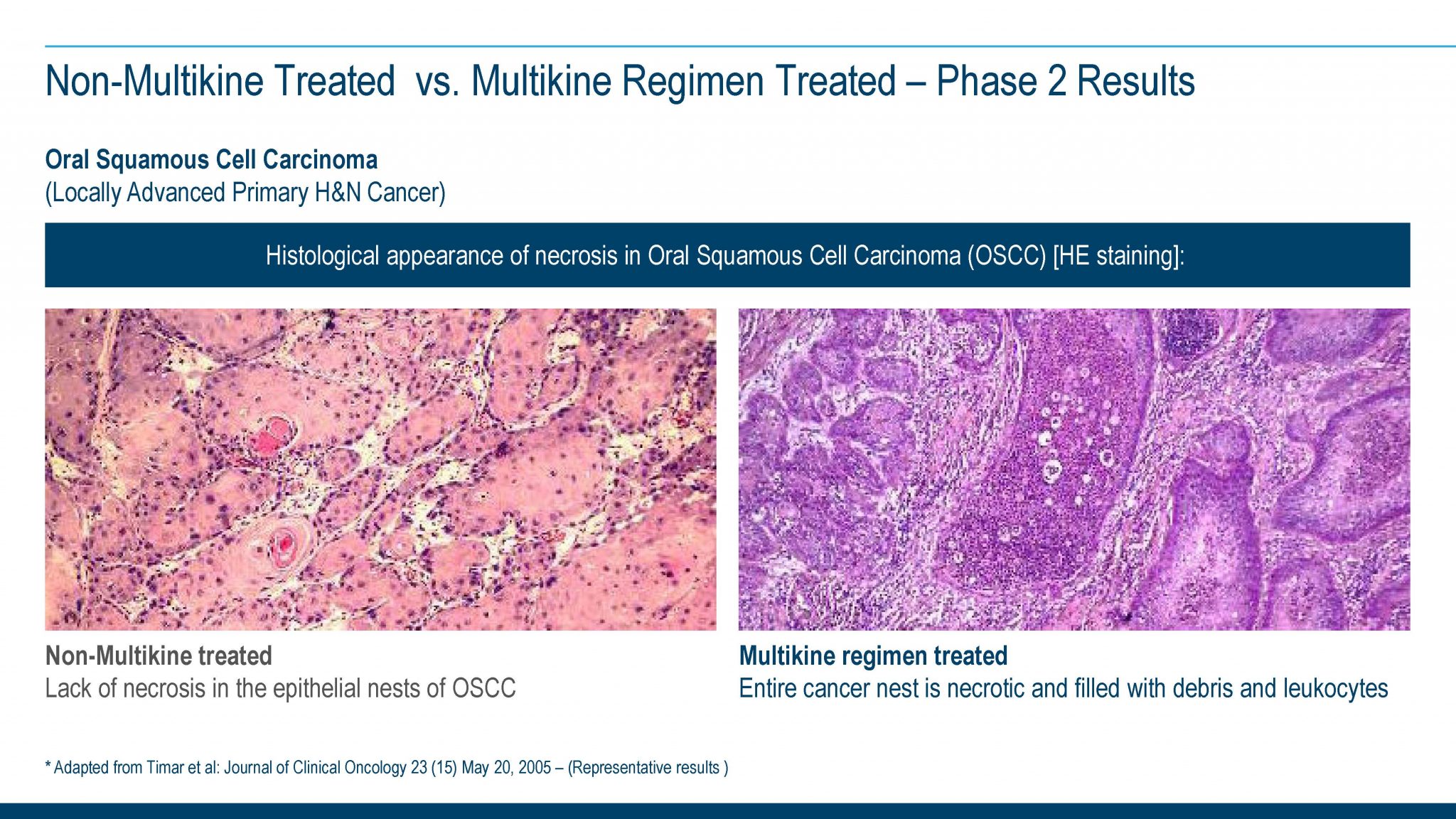
- Multikine potentially may directly affect/kill cancer cells:The various cytokines present in the Multikine investigational therapy, such as TNF, IL-2, IFN along with other cytokines, could be responsible for this potential activity.
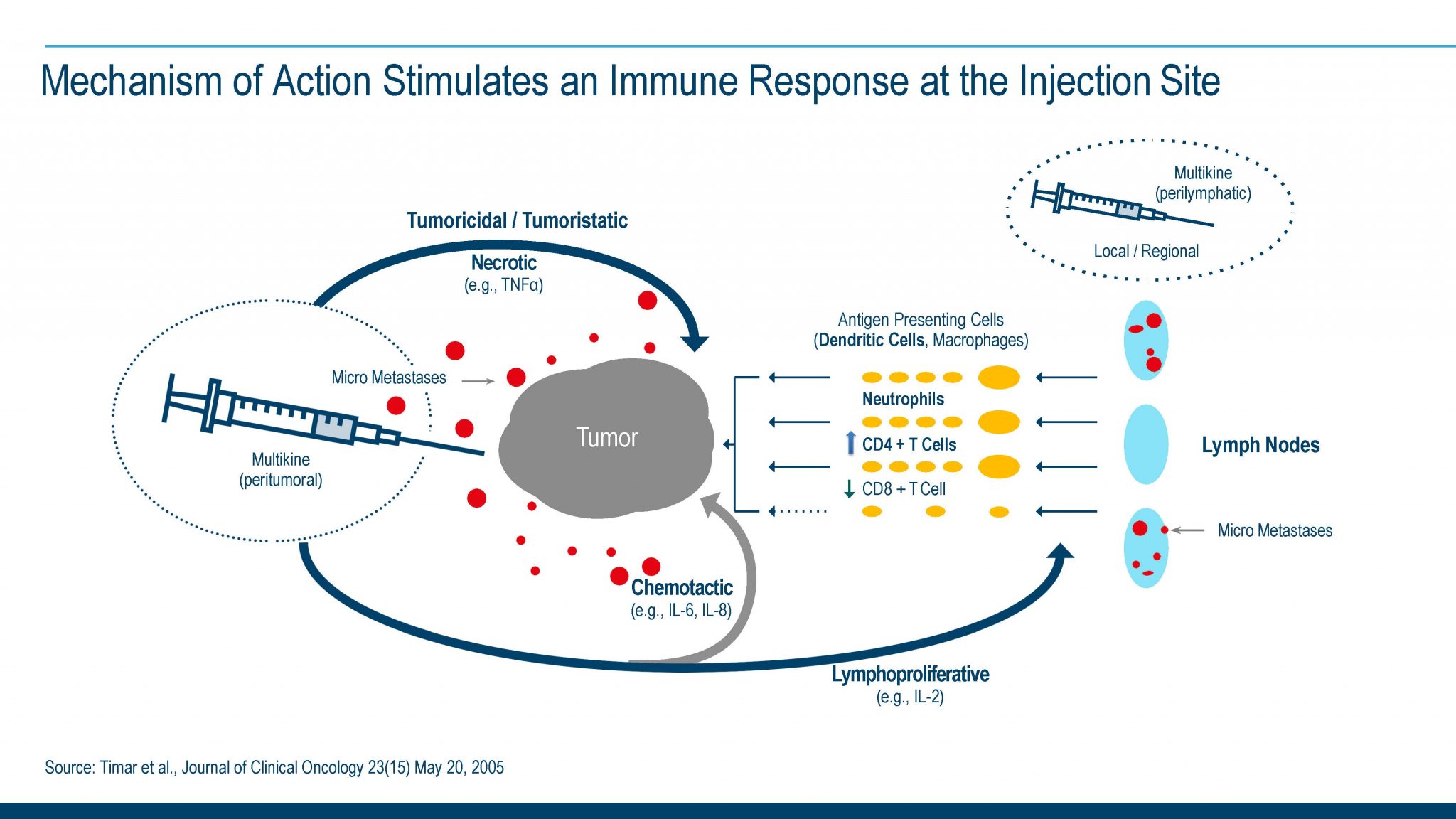
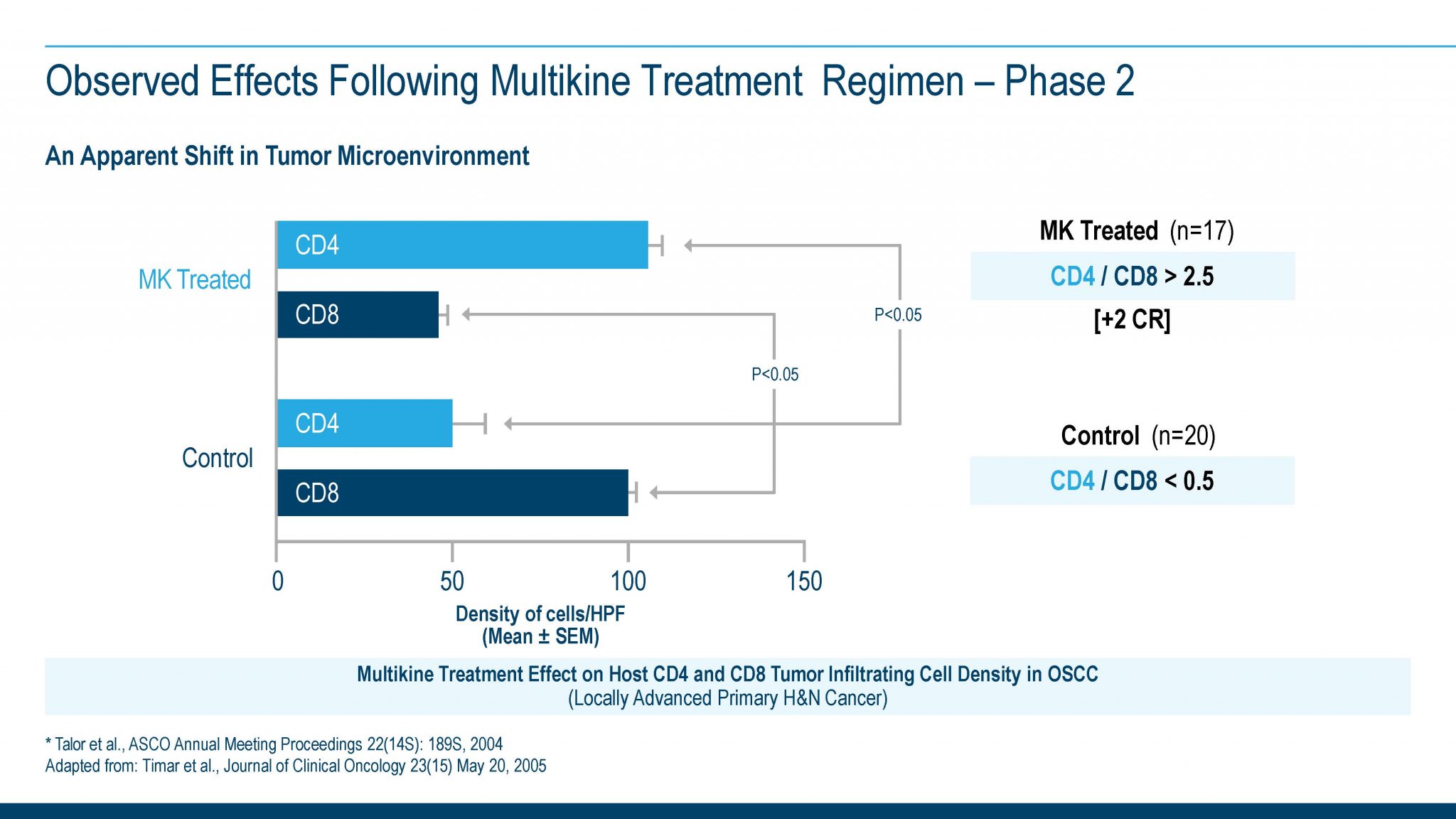
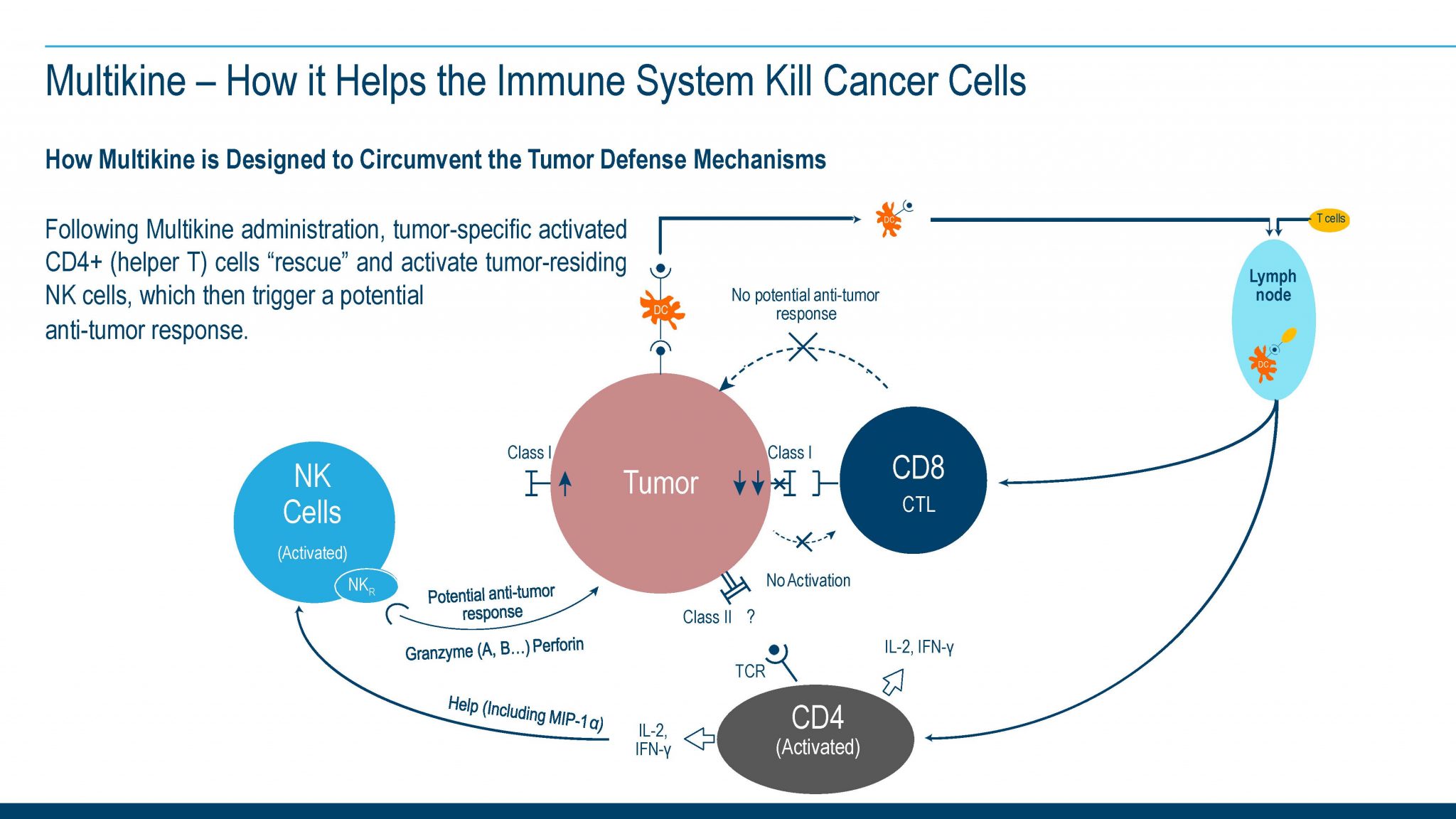
- Multikine may signal the immune system to produce an anti-tumor immune response: Pathology data from clinical specimens (reported from Phase 2 studies) also suggest that Multikine could change the type of cells that infiltrate and attack the tumor from CD-8 cells to predominantly CD-4 cells. These CD-4 cells have the potential to bring about an anti-tumor immune response to the tumor microenvironment (Timar et al 2005).
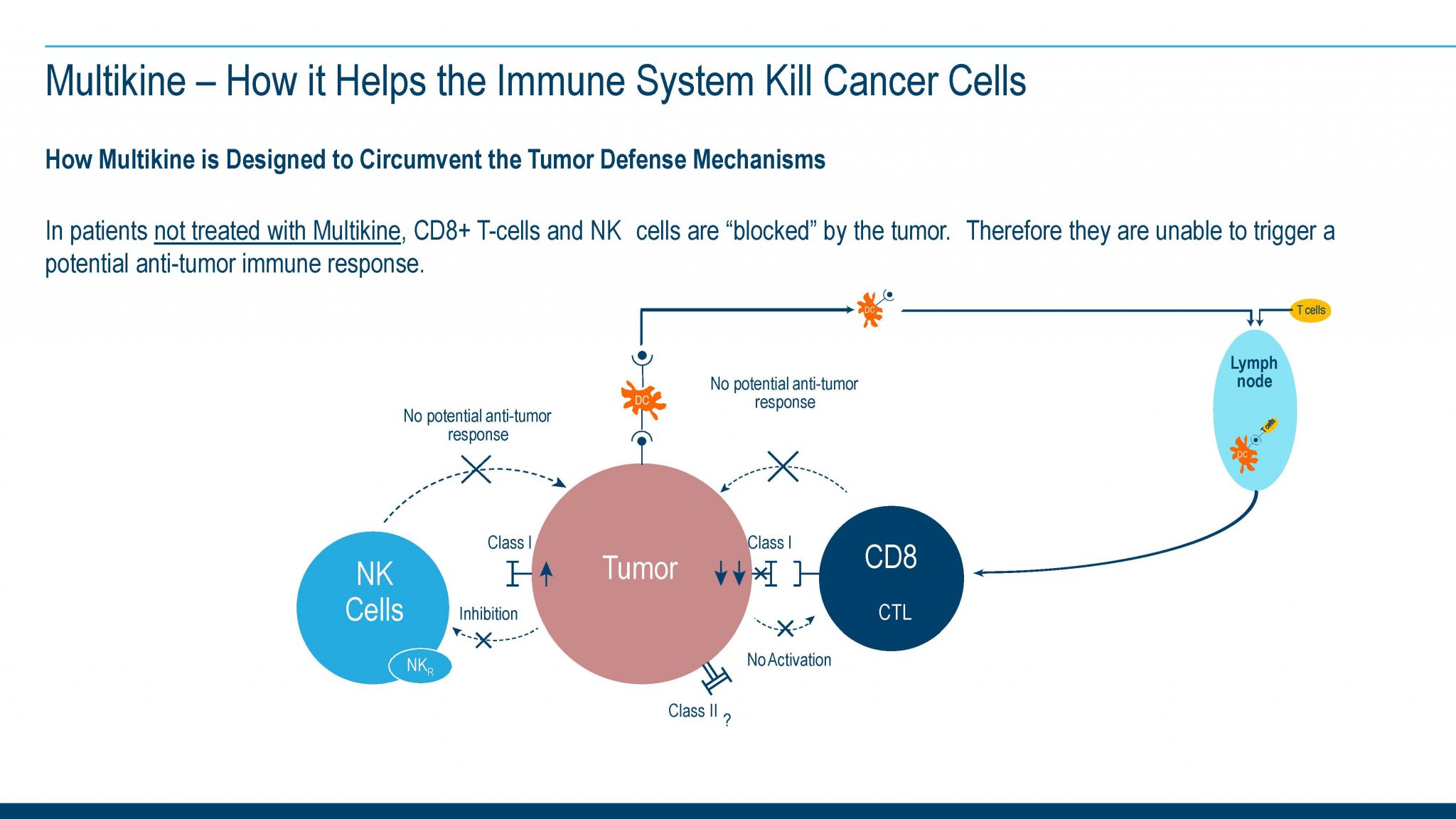
- Although the clinical significance of such a response if confirmed is not yet established, this could be important because the tumor is able to shut down the infiltrating CD-8 cells, but preliminary evidence seems to suggest a potential inability to shut down the CD-4 cell. In addition, preliminary data suggests that CD-4 cells appear to help break “tumor tolerance,” thereby potentially allowing the immune system to recognize and address the tumor. The normal immune system is made ‘blind’ to tumor cells, in part, because the tumor cells are derived from the body’s own cells, and thus the body ‘thinks’ of the tumor as ‘self’, a phenomenon also known as ‘tumor tolerance’.
- Multikine may have the potential to render the remaining cancer cells susceptible to radiation and chemotherapy treatment (Timar et al 2003).
Potential effect on recurrence of cancer: Tumor cells can persist after treatment with radiation, chemotherapy and surgery. The persistence of tumor cells is believed to be partly responsible for cancer recurrence.
The Multikine investigational therapy is injected around the tumor and in the vicinity of the draining local lymph nodes because these are the areas in which metastases are believed to most likely develop and where the cancer may recur in most cancer patients with this disease. Preliminary data from early-phase studies and support from survival data derived from the Phase III study suggest that the Multikine investigational therapy possibly could enable the immune system to have a potential anti-tumor response before tumor recurrence can occur or if it recurs it may be better able to “keep it in check”. The following depicts CEL-SCI’s current understanding based on available and published data of how this may occur. The hypotheses represented in these figures were formulated from and depict the clinical and pathology data collected during Phase I and Phase II clinical trials (Timar et al 2003 and 2005), and our current understanding of these preliminary data. The completed Phase III trial tested the hypothesis that Multikine treatment, administered prior to standard of care treatment regimen, will improve overall survival as compared to SOC only treated control, enhance the local/regional control of the disease and reduce the rate of disease progression in patients with squamous cell carcinoma of the head and neck. CEL-SCI’s Phase III trial is designed to develop the substantial evidence required by FDA to definitively establish that Multikine is a useful drug to treat head and neck cancer. A large amount of pathology data has also been collected during this trial to confirm the Phase I and Phase II pathology findings and prove CEL-SCI’s understanding of how Multikine may possibly bring about its effects.
* Multikine is the trademark that CEL-SCI has registered for this investigational therapy, and this proprietary name is subject to FDA review in connection with our future anticipated regulatory submission for approval. Multikine has not been licensed or approved for sale, barter or exchange by the FDA or by any other regulatory agency. Similarly, its safety or efficacy has not been established for any use.